 Slashdot Mirror
Slashdot Mirror
Domain: heart.org
Stories and comments across the archive that link to heart.org.
Comments · 20
-
Re:Coud be that women lie more to male doctors
I remember reading somewhere that some conditions - particularly heart attacks - present differently between men and women. We typically think of chest pain and burning around the upper-left chest and shoulder area with a heart attack. Symptoms in women are often that and more - they might experience jaw/back pain, nausea and shortness of breath. Things that could be confused with a common cold or flu pretty easily.
It's the docs job to know the symptoms and correlate, they can't help much if they don't know the whole picture.
-
Re:Could it possibly be age?
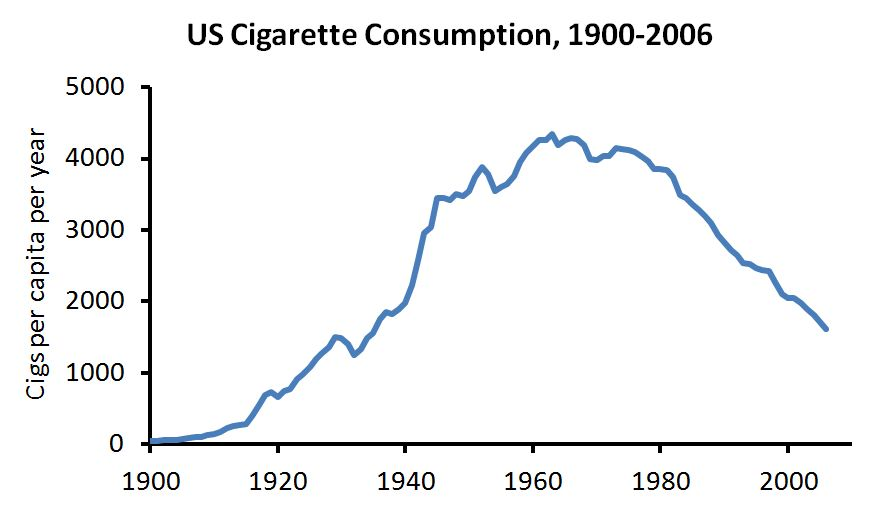
Also, there is a very interesting graph on the previous page depicting the AMI-related deaths for both sexes, with female deaths due to cardiovascular faults being in sharp decline since 2000. So either something happened around that time that made women less susceptible to dying from a heart attack, or something else took over as the big lady killer.
Here is the same graph (not divided by gender, though). The trend increases and decreases, To some degree matching cigarette consumption over the same period. Of course medical care has improved also over that time. Male cigarette smokers dropped more sooner, and farther, than women. There were more male smokers, too, so they had farther to drop. Currently rates between the two are the same.
The link between cigarettes and heart disease doesn't explain everything but it does explain a lot. -
Food Pyramid
Now it cones out = we all need to watch our diet = with respect to who's guidance?
The USDA Food Pyramid?
The American Heart Association's Diet and Lifestyle Recommendations?
American College of Cardiology
The USDA food Pyramid was built as much as a marketing tool for the food industry as it is a nutrition guide.
You could try this Japanese Health and Nutrition information but there is no way to tell if it is actually better, or if the users that make that claim are suffering from confirmation bias. -
Re:Eat Fat, Get Thin -- Refined carbs makes you fa
Since you don't seem to be able (or willing) to google this, here are a few results from the first page:
http://www.heart.org/HEARTORG/...
http://cardiobrief.org/2016/11...
https://www.hsph.harvard.edu/n...
Note that these are from science based publications... not fake news sites.
Also, animal saturated fat causes cancer:
http://www.pcrm.org/nbBlog/ind...
-
Re: And the next food craze starts
As for what AHA says about saturated fat, link.
In particular, the end:
There’s a lot of conflicting information about saturated fats. Should I eat them or not?
The American Heart Association recommends limiting saturated fats – which are found in butter, cheese, red meat and other animal-based foods. Decades of sound science has proven it can raise your “bad” cholesterol and put you at higher risk for heart disease.
The more important thing to remember is the overall dietary picture. Saturated fats are just one piece of the puzzle. In general, you can’t go wrong eating more fruits, vegetables, whole grains and fewer calories.
When you hear about the latest “diet of the day” or a new or odd-sounding theory about food, consider the source. The American Heart Association makes dietary recommendations only after carefully considering the latest scientific evidence.
Yes, because recommending eating "fruits, vegetables, whole grains and fewer calories" is totally a recipe for "almost single-handedly made America obese". Damn those fattening fruits, vegetables, whole grains and reduced-calorie diets.
-
Re:Shows the lengths....
Wait. The official cause of death is listed as Cardiovascular Disease and I'm the one who's reaching? I never said lung cancer didn't contribute to it, just that the official reason is heart failure and saying she died of lung cancer is perpetuating a myth.
There is ample evidence showing smoking increases the risk of Cardiovascular Disease, so it's safe to say that smoking contributed to her death, just not in the manner you described.
I suppose "cardiovascular disease" or "heart failure" don't have the same emotional impact as "lung cancer"...
-
Re:Brace for shill accusations in
It's from the National Academy of sciences, so you are in denialist class denial if you don't give it some credence.
I've been over this with the anti-GMO crowd before. There are actually a lot of organizations, ranging from government to nonprofit organizations, that are very much in favor of GMO technology. However each time you list one of them, the anti-GMO crowd comes up with some excuse as for why they're not trustworthy. Here's a list I can name off of the top of my head:
World Health Organization
Food and Agriculture Organization of the United Nations
U.S. Academy of Sciences
American Medical Association
American Heart Association (Nifty little tidbit I might add: http://newsroom.heart.org/news... but don't let any anti-GMO people see this or else they'll think the AHA is in on the Monsanto conspiracy as well.)
Girl Scouts of AmericaThe last one in that list is particularly interesting. Why? Because they've been the target of change.org petitions and massive parental protest against what is perhaps their biggest source of income: cookies. And yet still they remain steadfast in their opinion that, indeed, GMO is safe.
And you know what? I happen to agree. I also don't have any financial interest in GMO or any other agriculture, nor do I work for one. In fact I actually work for a major non-profit health care provider. I also happen to believe that GMO will eventually completely solve issues like world hunger and foodborne illness, and possibly even chronic disease as well.
-
Re:The top ads are the worst
OK, so there's an issue about ads getting embedded in search results, but, I see what you did there - embedding an ad in your comment. Perhaps that kind of sneaky embedding is why a search for acls.net has a "Fraud Warning - American Heart Association" show up so prominently just below your website. http://www.heart.org/HEARTORG/...
-
Re:First world problems...
What crack are you smoking, and where does someone get some?
So if something has 0% trans fat (for example), it can legally contain trans fat (in U.S.A.)
No, 0% means 0%, not 0.1%.
What crack are you smoking, and where does someone get some?
So if something has 0% trans fat (for example), it can legally contain trans fat (in U.S.A.)
No, 0% means 0%, not 0.1%.
Well, when it comes to nutrition labels, 0% means anything under 0.5%, because they can round off to the nearest percent: When the Nutrition Facts label says a food contains “0 g” of trans fat, but includes “partially hydrogenated oil” in the ingredient list, it means the food contains trans fat, but less than 0.5 grams of trans fat per serving. So, if you eat more than one serving, you could quickly reach your daily limit of trans fat. (American Heart Assoc.)
-
Re:GOOD GRIEF!By the way, don't believe me. Refer to the professional scientific consensus:
FDA:
Is HFCS less safe than other sweeteners?
FDA receives many inquiries asking about the safety of HFCS, often referring to studies about how humans metabolize fructose or fructose-containing sweeteners. These studies are based on the observation that there are some differences between how we metabolize fructose and other simple sugars.
We are not aware of any evidence, including the studies mentioned above, that there is a difference in safety between foods containing HFCS 42 or HFCS 55 and foods containing similar amounts of other nutritive sweeteners with approximately equal glucose and fructose content, such as sucrose, honey, or other traditional sweeteners. The 2010 Dietary Guidelines for Americans recommend that everyone limit consumption of all added sugars, including HFCS and sucrose.
The American Heart Association (AHA) recommends limiting the amount of added sugars you consume to no more than half of your daily discretionary calories allowance. For most American women, that's no more than 100 calories per day, or about 6 teaspoons of sugar. For men, it's 150 calories per day, or about 9 teaspoons. The AHA recommendations focus on all added sugars, without singling out any particular types such as high-fructose corn syrup.
(FYI -- that daily limit for sugar for men is approximately one 12-oz. can of soda. It's less for women. And that assumes you don't consume ANY added sugars in anything else you eat that day, which is nearly impossible if you consume any processed foods.)
Review article supported by the American Medical Association:
Because the composition of HFCS and sucrose is so similar, particularly on absorption by the body, it appears unlikely that HFCS contributes more to obesity or other conditions than sucrose does. . . . At the present time, there is insufficient evidence to ban or otherwise restrict use of HFCS or other fructose-containing sweeteners in the food supply or to require the use of warning labels on products containing HFCS. Nevertheless, dietary advice to limit consumption of all added caloric sweeteners, including HFCS, is warranted.
You can find plenty more things like this if you look, because there are dozens of studies that back up such a position. After decades of looking, we so far have only a handful of studies measuring significant differences with HFCS metabolism. That doesn't mean we shouldn't keep looking... but it's important to see those Princeton findings in context.
-
Re:its a drug bust
Yes, but whose lives are ruined? The lives of the people who choose to take such drugs.
My guess is you haven't had to deal with a family member who is permanently paralyzed on one side from several strokes during heart surgery which was needed after decades of doing crack and abusing prescription drugs, who will never get better and will die a premature death.
How does cocaine affect the heart?
Cocaine use kills over 15,000 people each year in the United States due to overuse or related accidents. Additionally, cocaine use can cause damage to the heart, which leads to many more deaths each year. Several cardiovascular complications are closely related to cocaine use. They include chest pain syndromes, heart attacks, heart failure, strokes, aortic dissection, and fatal and nonfatal arrhythmias.
Others include:
myocarditis (inflammation of the heart muscle)
endocarditis (inflammation of the inner lining of the heart)
pulmonary edema (fluid in the lungs)
vascular thrombosis (blood clots in blood vessels)
dilated cardiomyopathy (an enlarged heart)Some of these potentially fatal complications can occur in a first-time user. Older people with abnormal coronary arteries and diseased blood vessels in the brain are at even greater risk.
Today law enforcement agencies and the medical community recognize cocaine as one of the most dangerous illicit drugs in common use. Because it's increasingly popular and easily bought, the number of cocaine-related cardiovascular disabilities and deaths may be expected to rise. Furthermore, smoking crack cocaine, which is cheaper, more potent and widely available, will lead to even more strokes and heart attacks in younger people not normally "at risk."
It's going to cost taxpayers at least $70k a year (on top of the 6-figure sum already spent last year for quintuple bypass, physiotherapy to try to restore function, etc) because she needs 24/7 care in an institutional setting and frequent doctor's visits, so it affects everyone. And that's not factoring the impact on family and friends.
-
Re:People are the problem
Not to mention that a) defibrillation alone without medication and oxygen has a very low success rate and b) not all cardiac dysrhythmias respond to defibrillation. And not all pulseless patients are having a heart attack. Try defibrillating a brain aneurysm or a pulmonary embolism and see what you get. Just like the defibrillators in airports - how many have been used successfully to date? This is good news only for companies that sell defibrillators.
I am an Emergency Room RN, with 8+ years of experience, including Advanced Cardiac Life Support.
Most of the research of which I'm aware shows that early defibrillation is second only to good CPR in the vast majority of cases. Studies from Japan have showed that the most common medication, epinephrine, actually does nothing more than allow a body to get to the hospital with a non-functioning brain, but it has been used for so long by out of hospital providers that it is a very difficult thing to remove from the protocols ("but, we have to do something!") Oxygen is also being stressed less, as research shows that it can cause vasoconstriction of the coronary arteries.
Out of hospital survival rates for cardiac arrest are lower than most people think (as are in-hospital rates, though they are higher. See http://www.heart.org/HEARTORG/... for U.S. statistics). The reason for higher survival rates in the hospital setting are varied, but the biggest reason is that you have trained people nearby, and quick access to the one thing that makes a real difference - early defibrillation of an appropriate arrhythmia.
Early AED delivery in the field could be of great assistance in the right circumstances.
BTW, an AEDs do not recommend defibrillation unless it senses a "Shockable Rhythm," i.e. Ventricular Tachycardia or Fibrillation. OP is correct that there are other rhythms which do not respond to defibrillation, but a) AEDs are good at recognizing them, and b) rates of survival to neurologically-intact discharge are much lower, on the order of a full order of magnitude. A patient with Pulmonary Embolus or Aneurysm (or Seizure for that matter) would not have either of these rhythms.
-
Re: I can simply ignore all health and diet advice
American Heart Association stance on trans fats: http://www.heart.org/HEARTORG/... . They are just used because they are cheap and highly shelf stable. Are they on the same realm as smoking? Not quite, but people "like you" were probably the last to admit smoking was bad.
-
The best reason for alternative energy
If we can make alternative energy work, that is.
Oil is... it's great, but there's a high cost, mainly air pollution which may cause autism and heart disease among other problems.
The spills are disasters which cause ongoing problems for decades if not longer.
In addition, the scarcity of the resource makes future wars, politics, etc. inevitable.
I'm looking for one of those reactor-type-devices from the end of "Back to the Future" that can deconstruct ordinary household waste and produce high amounts of energy. Were I President of the ol' USA, I'd slam resources into that before anything else but space exploration.
-
Re:Why single out Whole Foods?
- One... iodine does NOT come with sea salt OR mined salt. All salt has to be fortified with iodine if you want iodine in it.
- Two... people NEED iodine in their food. It is ABSOLUTELY necessary in our diet to prevent goitre and more importantly to prevent cretinism. The human race took a HUGE jump in intelligence when salt began being iodized. It is easy to see families who buy into all the bullshit and decide iodine is not good for you. They are the stupid ones.
- Three... ALL salt that we use is sea salt. The salt that is mined from under the ground comes from seas that evaporated a long fucking time ago. Table salt == sodium chloride... whether you get it as the residue of freshly evaporated sea water, or sea water that evaporated a long time ago.
- Four... you don't get much if any benefit from the 'extra' minerals in 'sea salt'. It has the same sodium content as mined salt, and since the amount of these minerals are found in much higher quantities in the food the salt goes on, the amount in the salt is moot.
- Five... the difference is usually more a matter of taste. But get iodized sea salt if you like it better.
-
Re:When should you trade saturated for trans?
No it isn't. You may have noticed how people have become less healthy as they removed saturated fats from their diet. You may however missed the vast body of evidence that has replaced the crappy epidemiological evidence that wrongly implicated saturated fats in the 70s.
Really. Let's see a few more recent studies, then.
No. This is the thoroughly debunked consensus. It is not longer consensus.
Well then, let's see what major medical and health associations say, then:
- The American Heart Association: (1)
- The Center for Disease Control: (1)
- The European Food Safety Authority: (1)
- The World Health Organization: (1) (2)
It's ketogenic. The metabolic pathways that make this true are fully understood.
Okay, cool beans. Feel free to explain the pathways and why more ketones is a good thing.
-
Re:And yet...
Guns amplify the problem like no other tool in existence does.
So yeah easy access and possession of guns IS THE FUCKING PROBLEM.Gun homicides in the US ~ 9000/year (2010).
AIDS deaths a year, 17,000/year
2009 vehicle accident deaths 33,808/year.
Smoking releated deaths 440,000/year.
Cardiovascular diseases kill 2,140 a day or ~800,000/year.
Sure looks like guns make the lions share of the killing. -
Re:Pool ressources
And in America, one in three children are overweight or obese.
Should we call back Curiosity? -
Re:Congrats!
Given that X-rays are used as a part of the follow-up care when implanting pacemakers, I wouldn't worry about X-rays in particular. Google also has some academic studies if you're interested.*
What I'd be more worried about-- and this is perhaps on my mind more than most people, because the laboratory I work in studies just this-- is whether the digital components are hardened against malicious attackers. My colleagues' preliminary results suggest that the answer is no-- these things are quite hackable.
* one caveat: this was discovered by a professor here. -
Re:Emergency Medicine Protocols
The AHA's current guidelines page is here. A good quick summary for recent changes is the 'Summary of Changes' document which covers the changes from community to skilled provider CPR. http://www.heart.org/presenter.jhtml?identifier=3
0 35517
When big changes in the AHA guidelines happen, they are usually published in a special edition of Circulation. That has the details ad nauseum. http://circ.ahajournals.org/content/vol112/24_supp l/
Before I was an ER physician, I was an EMT. I didn't have as much clinical information as I do now, but I was able to think for myself. One particular event comes to mind... in the book Brady Emergency Care (the text for most EMT courses) it tells you that if possible, if the person has vomiting or diarrhea, you should try to transport the effluent to the hospital.
I was stuck working with another EMT who was (literally) a sorority girl who was a sophomore pre-med at UNC. We were up in the back woods of Orange County (20 miles and 50 years from Chapel Hill) and had a call at a house with no indoor plumbing. The teenage daughter had a bad stomach flu. Unfortunately without a toilet, the family facilities (in winter) was a 5 gallon plastic cement bucket on the back porch (filled about 2/3 full with excrement of various family members.) Ms Alpha Kappa Dumbass decides we must take the bucket of shit and piss to the ER. Arguing with her that A) their were multiple samples of people's shit in said bucket, B) the bucket would spill and smell on the 20 mile ride, and C) no ER nurse would ever let me live this down if I walked in with that bucket'o'turds.... were all quite meaningless in light of her photographic memory of Brady Emergency Care's dictum.
Ultimately I just gave up and told her I would drive, she could do what she wanted, but if that shit spilled SHE would clean it up.
The predictable thing happened, and by arrival at UNC Hospitals, we had a 1/3 full cement bucket which had been 2/3 full. Ms Alpha Kappa Dumbass (now smelling of shit to high heaven) marches in with the bucket and the stretcher. I was literally physically incapacitated and had to sit on the floor as the triage nurse had the most entertaining (yet incredibly short) conversation with this idiot.
The morals of this story are that 1) you are better off knowing why you are doing something than memorizing rote procedure and 2) someone who thinks things through rather than carrying 3 gallons of shit and piss to the ER is the one that gets to take an hour lunch break while the unit is 10-7 as the ignorant sorority chick gets to scrub shit out of the ambulance. Same thing with this argument. You are better off with a thinking EMT helping you who will be able to take basic concepts and expand them to fit the situation.
In addition teaching that a protocol that is at best evolving to be somewhat evidence based is infallible will make it a while lot harder to retrain people if they think they learned the absolute truth a decade ago.
-Nick
{kind=link}
{kind=link}